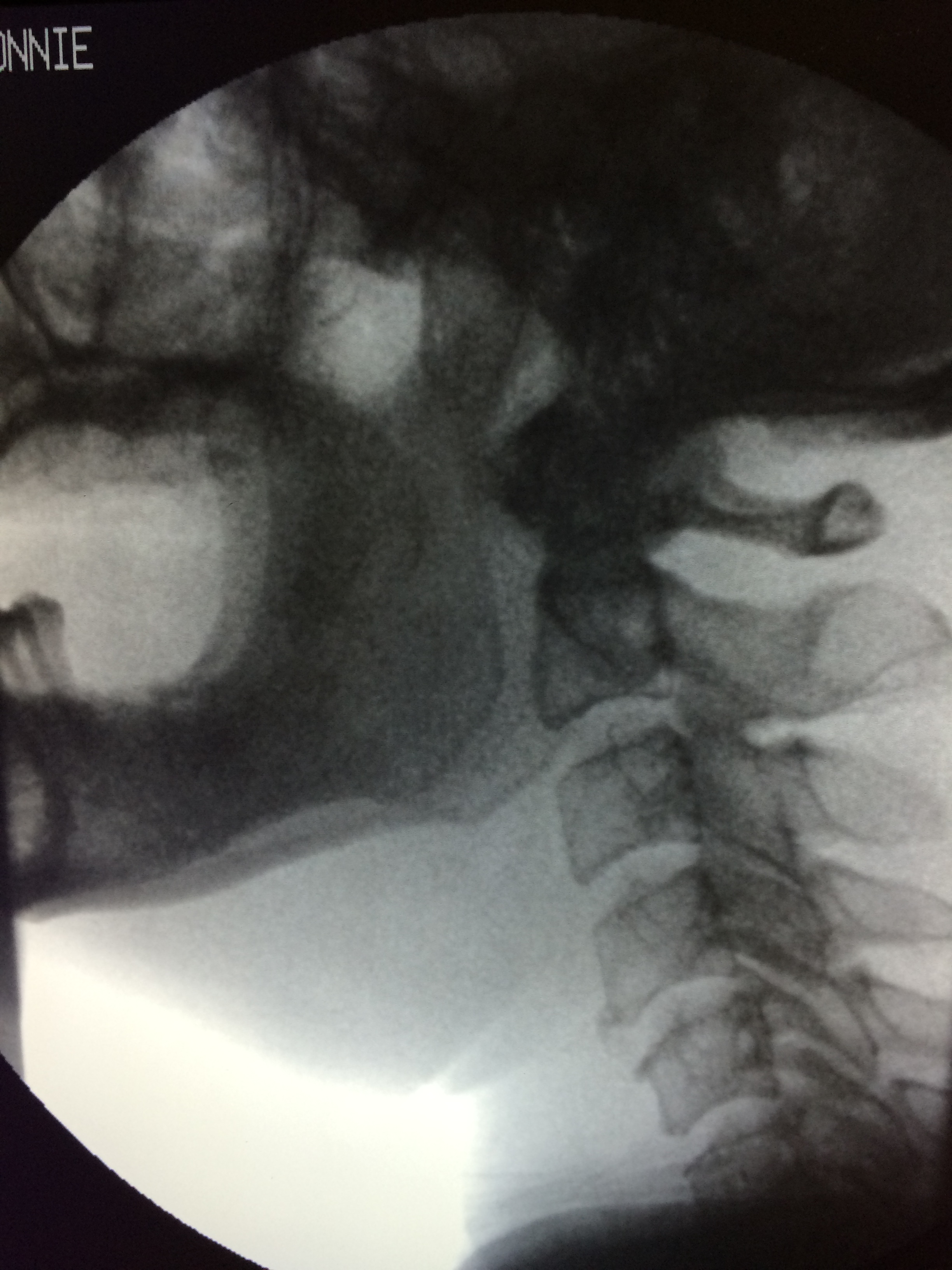
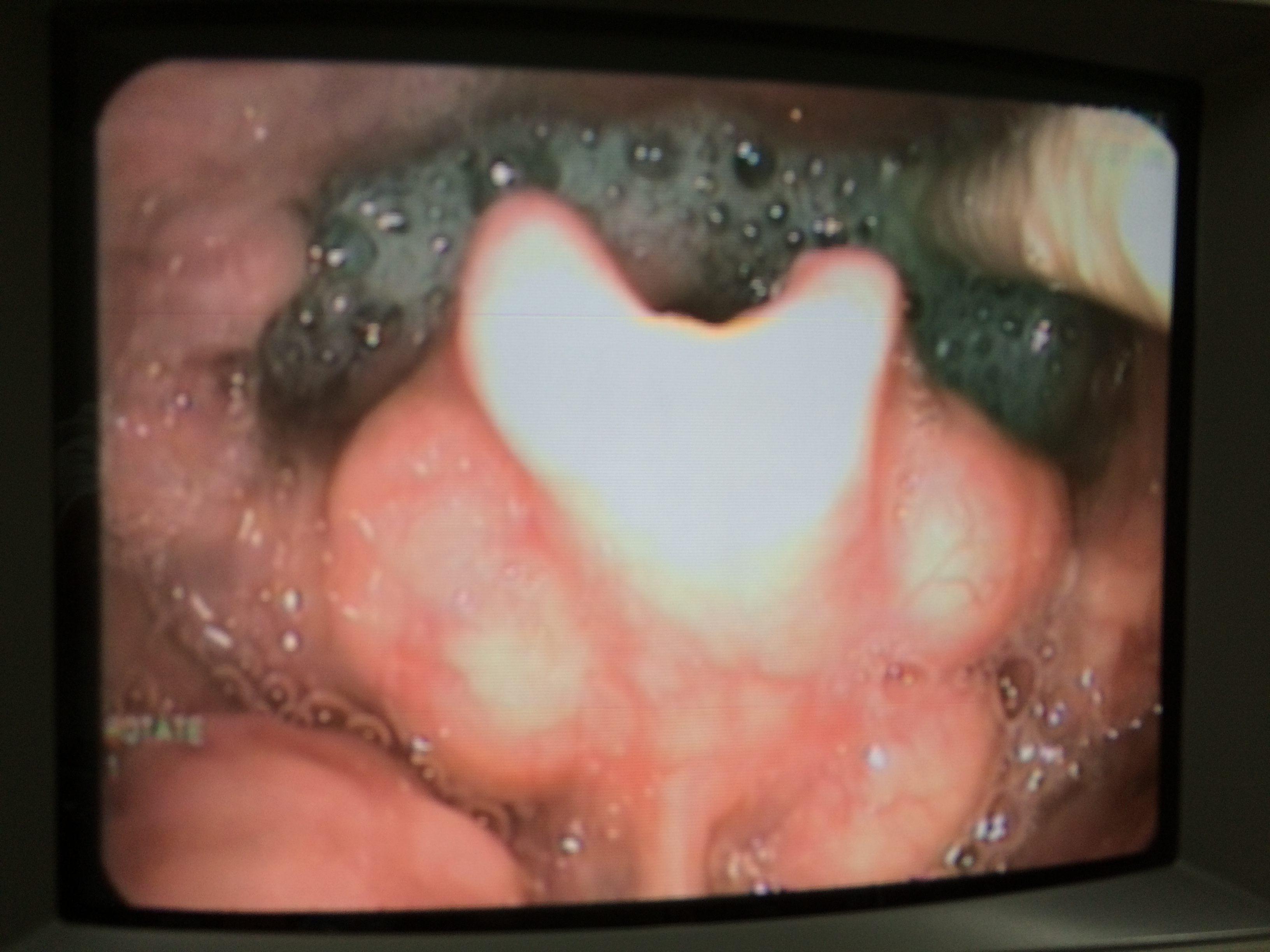
I will be conducting a talk titled Videofluoroscopy (VFS) Interpretation Made Easy for Speech-Language & Hearing Association Singapore.
Date: 24 April 2015 (Thursday)
Time: 6.15pm – 8.30pm
Venue:
National University Hospital
Group Therapy Room, Main Building Level 1,
5 Lower Kent Ridge Road, 119074
About this talk:
This talk is a short introduction to Videofluoroscopy (VFS) interpretation and is suitable for both clinicians who are experienced or inexperienced in performing VFS. I will introduce pathophysiologies commonly viewed in VFS with the use visual examples. I will also share on how I analyze VFS systematically, and how to select suitable strategies to be trialed during the procedure accordingly to patient’s presentation.
Outline of the talk:
Short introduction about VFS
Pathophysiologies viewed in VFS
Esophageal phase screening
How to interpret VFS systematically rienced clinicians to share their experiences and views on VFS as well rienced clinicians to share their experiences and views on VFS as well.
In March 2013, Mr Jason Khoo (A MSc SLP graduate from NUS) presented this scientific poster on CTAR at the Dysphagia Research Society Meeting at Seattle, Washington, USA in 2013. Little did we expect that CTAR actually drew so much interest at the DRS meeting and was also awarded first place for the Scientific Abstract Poster.
CTAR was awarded first place in Scientific Abstract Poster at DRS 2013
Comparison of suprahyoid muscles activity between chin-tuck-against-resistance (CTAR) and the Shaker exercises
Jason KHOO, Susan J. RICKARD LIOW, YOON Wai Lam
Summary
For patients with pharyngeal dysphagia, therapeutic exercise such as the Shaker exercise to strengthen the suprahyoid muscles is effective in restoring oral feeding. However, observations revealed that the Shaker exercise is physically demanding for the elderly patients, thereby affecting compliance of the exercise goals. A less strenuous exercise, CTAR, was compared to the Shaker exercise by measuring the surface electromyography (sEMG) activity of the suprahyoid muscles during both exercises. The sEMG activity of the suprahyoid muscles during CTAR was similar or superior to the Shaker exercise. Therefore, CTAR exercise has the potential to achieve the same therapeutic effect as Shaker exercise and may improve compliance.
Introduction
Aim: To find out if CTAR is as effective as Shaker exercise in exercising the suprahyoid muscles.
The Shaker exercise has been shown to be effective for patients with dysphagia due to incomplete upper esophageal sphincter (UES) opening (Shaker et al, 2002).
Performing Shaker exercise significantly increased the anteroposterior diameter of the UES (Easterling et al, 2005) and significantly reduced post-swallow aspiration (Logemann et al, 2009).
A key component of Shaker exercise is in exercising the suprahyoid muscles, thereby strengthening it (Shaker et al, 2002).
Easterling et al (2005) found out that muscle discomfort or time constraints were main reasons for the failure of their participants in attaining the Shaker exercise goals.
Clinical observations suggest the Shaker exercise may pose a physical challenge for elderly dysphagic with chronic disease (Yoshida et al, 2007).
Developing a less strenuous therapeutic exercise would potentially benefit patients who find Shaker exercise physically challenging, thereby facilitating the attainment of the exercise goals.
The CTAR exercise, performed in a seated position, is less strenuous as the patient is not required to lift the weight of her head.
Performing the CTAR exercise in a seated position would make it more convenient for dysphagic patients who are actively mobile to comply with, thereby improving compliance.
The CTAR will adopt the same regime as Shaker exercise; a set of isometric (sustaining the effort) and isokinetic (repetitions) exercise with equal time base.
Research question: Would the sEMG activity of the suprahyoid muscles be higher during CTAR exercise?
Method
Participants:
N=40 healthy adults (21-40 yrs). Each participant performed a total of 4 exercise tasks, with a minimum 5 minute rest in between each task. The order of the 4 tasks are randomly assigned and counter-balanced across participants.
4 exercise tasks:
CTAR isometric
CTAR isokinetic
Shaker isometric
Shaker isokinetic
CTAR exercise (see Figure b):
Seated upright in chair
An inflatable rubber ball (diameter 12cm) is placed between chin and base of neck to provide resistance
Chin tuck against the ball and sustaining it for 10 sec (isometric)
Chin tuck against rubber ball for 10 repetitions (isokinetic)
Shaker exercise (see Figure c):
Supine position
Lift head high enough to see their toes
Sustaining the head lift for 10 sec (isometric)
Lift head for 10 repetitions (isokinetic)
sEMG (see Figure a):
The activity of the suprahyoid muscles was measured using sEMG via an electrode patch attached to the participant’s suprahyoid area
Results
Discussion
The CTAR exercise appears to be similarly effective or superior to Shaker exercise in utilising the suprahyoid muscles.
If Shaker exercise is effective in strengthening the suprahyoid muscles and increasing the anteroposterior diameter of the UES, CTAR exercise may be able to achieve a similar or greater effect.
CTAR exercise may be a potential alternative for elderly dysphagic patients who find Shaker exercise physically challenging.
This study is limited to healthy young adults. Replication of this study on an older population will enable further understanding of the impact of age.
Future clinical studies are necessary to evaluate the therapeutic potential of CTAR in dysphagic patients with incomplete UES opening and the compliance of CTAR exercise amongst the elderly patients.
CTAR is top 10 most downloaded article in Dysphagia 2014
Chin Tuck Against Resistance (CTAR) is the top 10 most downloaded article from the Dysphagia Journal in 2014
I would like to take this opportunity to thank Speech-Language Pathologists / Therapists around the world for all the interest, support and word of encouragement for the Chin Tuck Against Resistance (CTAR) exercise and researches.
The National University of Singapore MSc SLP team will continue to try our best to come out with more quality researches.
The surprise news came from Mr Sze Wei Ping (A MSc graduate from National University of Singapore) 2 weeks ago when he went to present the follow up study on CTAR at the 23rd Dysphagia Research Meeting at Chicago, 2015. The first CTAR publication is actually the top 10 most downloaded article for the Dysphagia journal for year 2014.
Chin tuck against resistance (CTAR): new method for enhancing suprahyoid muscle activity using a Shaker-type exercise.Dysphagia. 2014 Apr;29(2):243-8. doi: 10.1007/s00455-013-9502-9. Epub 2013 Dec 15.
CTAR was awarded first place in Scientific Abstract Poster at DRS 2013
The interest on CTAR has started in Singapore long before it was announced to the world in 2013. In March 2013, Mr Jason Khoo (A MSc SLP graduate from NUS) presented the first scientific poster on CTAR at the Dysphagia Research Society Meeting at Seattle, Washington, USA in 2013. Little did we expect that CTAR actually drew so much interest at the DRS meeting and was also awarded first place for the Scientific Abstract Poster.
Some wrote in to enquire on how CTAR started?
Here is how it all begins….
The hunt for stretch ball was started in the year 2002 when I was still a junior SLP at Singapore General Hospital. I drew the inspiration from my geriatric patients who kept complaining that the Shaker’s exercise are too strenuous and they declined to perform it. After some thought, I came out with the idea of performing the chin tuck in a sitting position and conveniently use one of the stretch ball belongs to one of the patient and placed it under the patient’s chin as resistance. The geriatric patient was more willing to perform it and complaint of soreness felt at the chin area (Suprahyoid area) – that’s the sign of muscle fatigue! So I started to hunt for stretch balls on the very same night, bought at least 10 pieces. But I did not take into consideration the variation in neck length. The stretch ball was too small and hard for those with longer neck to hold it in between their chin and chest. A bigger ball was used (~10cm) and it seems to fit in nicely for most patients.
I actually prefer to use my palm to provide resistance. Why?
What about for patients who were just too weak to even initiate chin tuck with effort against the ball resistance? I noticed these patients were just resting their chin on the ball. I decided to use my palm to support the chin and found out that the effort for some of this patients were just so minimal as a result of their weakness. I did some search and found out from some dental journals indicated that the Suprahyoid muscles will only be activated when the chin is tucked down for at least 20 degrees, and the greater the degree, more suprahyoid muscle activities were noted. Also taking into consideration the principle of muscle strengthening, that for muscle to be strengthen, it has to be resisting about 60-80% of one repetition maximum. At least by using my palm I can estimate patient’s maximum effort and attempt to adjust my resistance accordingly to their effort (~60-80% of their max effort).
Outcome?
I have been performing CTAR for my patients for more than 10 years and I have seen good clinical outcomes in even severe dysphagia cases (i.e. lateral medullary syndrome).
Why I use a 12cm diameter ball in my study?
Making exercise easy and cost effective has always been my aim. The ball was chosen because it suits most neck length. Also, in research all subjects should be given the same type of resistance.
In the next coming blogs, I will be posting all the CTAR posters. Stay tuned!
Most patients have the perception that when they see or being referred to a speech therapist, they must receive some form of active treatment that involves active exercises. This may not be true all the time.
Why?
From speech therapy perspective, a medical diagnosis that explains the presentation of speech/ language/ voice / swallowing difficulties is required before any active therapy can be initiated.
That is because these difficulties are usually symptoms presented as a result of certain medical condition(s). For example, a new onset of swallowing difficulty is actually a symptom of neurological disorder(s) or brain related problem(s) that require further diagnosis by a neurologist. The causes may include stroke, neurodegenerative diseases, myasthenia gravis and etc.
Some active treatment may contraindicate the presenting medical diagnosis. For example, for myasthenia gravis (MG), the muscles will weaken further as one gets more tired/fatigue. As such strengthening exercises would not be appropriate for this condition. In fact, compensatory methods such as eating small amount but frequent meals if patient gets fatigue easily and unable to finish up full meal safely may be a better choice of management. In fact treatment for MG that has been shown to be more effective in improving functions include medical intervention and/or surgical intervention. Speech therapist plays the role in assessing suitability for oral feeding, teaching compensatory strategies and providing information counseling.
So for any presenting symptoms that do not associate with any preexisting medical diagnoses, perhaps the next best management is to refer the patient to see a medical specialist who can assess and potentially provide a diagnosis that may explain the presenting symptoms.
In summary, active speech therapy that involves exercises need not be the choice of management all the time especially if there is no confirmed medical diagnoses. Finding out the cause(s) of the symptom(s) / presentation(s) will allow us to make better clinical diagnosis which will lead to better management / treatment that is usually more cost effective. This is especially so with the rising cost of healthcare in Singapore and Worldwide.
Videofluorosocopy (VFS)FEES assessment of swallowingsEMG biofeedback as an adjuct to swallowing therapy
 Videofluoroscopy_Interpretation_Made_Easy_Registration_Form _1_
Videofluoroscopy_Interpretation_Made_Easy_Registration_Form _1_