A comprehensive dysphagia (swallowing disorders / difficulties) management is not only limited to diet recommendation, compensatory strategies or rehab exercises. Providing crucial feedback to the medical team is equally important.
The following case is one case example:
I was consulted by my speech-language pathologist / therapist colleague regarding a case of worsening dysphagia within days in a rehabilitation hospital. The patient (pt) had a stroke (left MCA infarct) diagnosed 2 weeks ago. According to the medical report from the acute hospital, the pt presents with global aphasia and dense right hemiplegia.
Day 1:
Initial assessment revealed mild oropharyngeal dysphagia and global aphasia. Delayed swallowing initiation was suspected. Meal supervision was performed by the ST and pt was started on soft diet and thin fluids.
Day 2:
Patient’s swallowing presentation appeared to have worsen. Oral control appeared poorer, and oral residues were noted post swallow. Noted reduction in hyolaryngeal elevation and double swallows per bolus. Coughed on thin fluids. Diet was downgraded to minced diet and nectar thick fluids by teaspoon.
Day 3:
Staff nurse reported to the ST that pt is coughing on minced diet and nectar thick fluids during breakfast. On ST review, it was noted that patient presents with tongue pumping with significant amount of oral residue post swallow, delayed swallowing initiation, and multiple swallows per bolus. Wet voice was noted post swallow.
I was asked by my colleague for a second opinion.
**Before I move on to explain our plan for the case, allow me to list down the suggestions by some of the SLPs I spoke to when I presented the case to them.
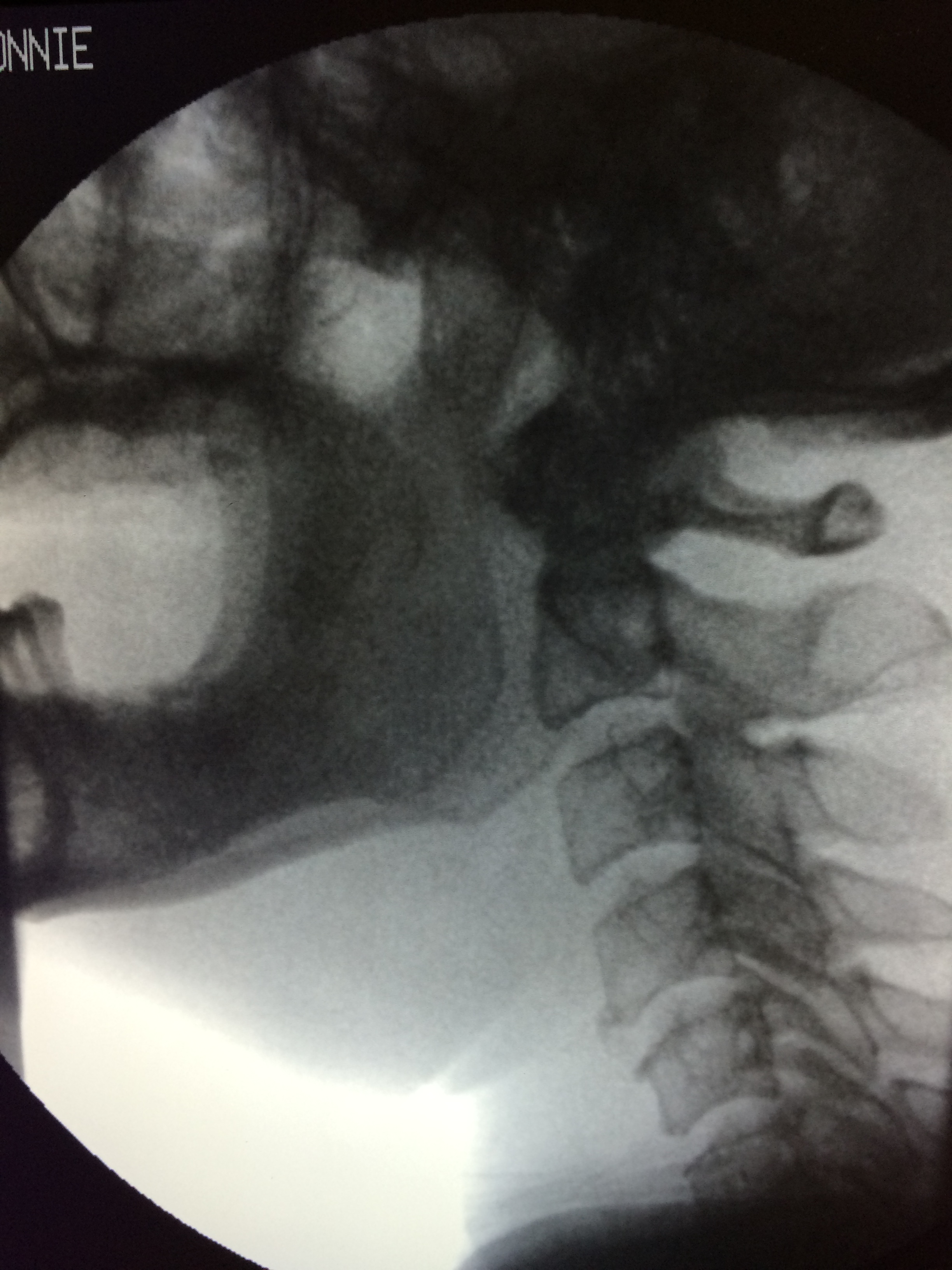
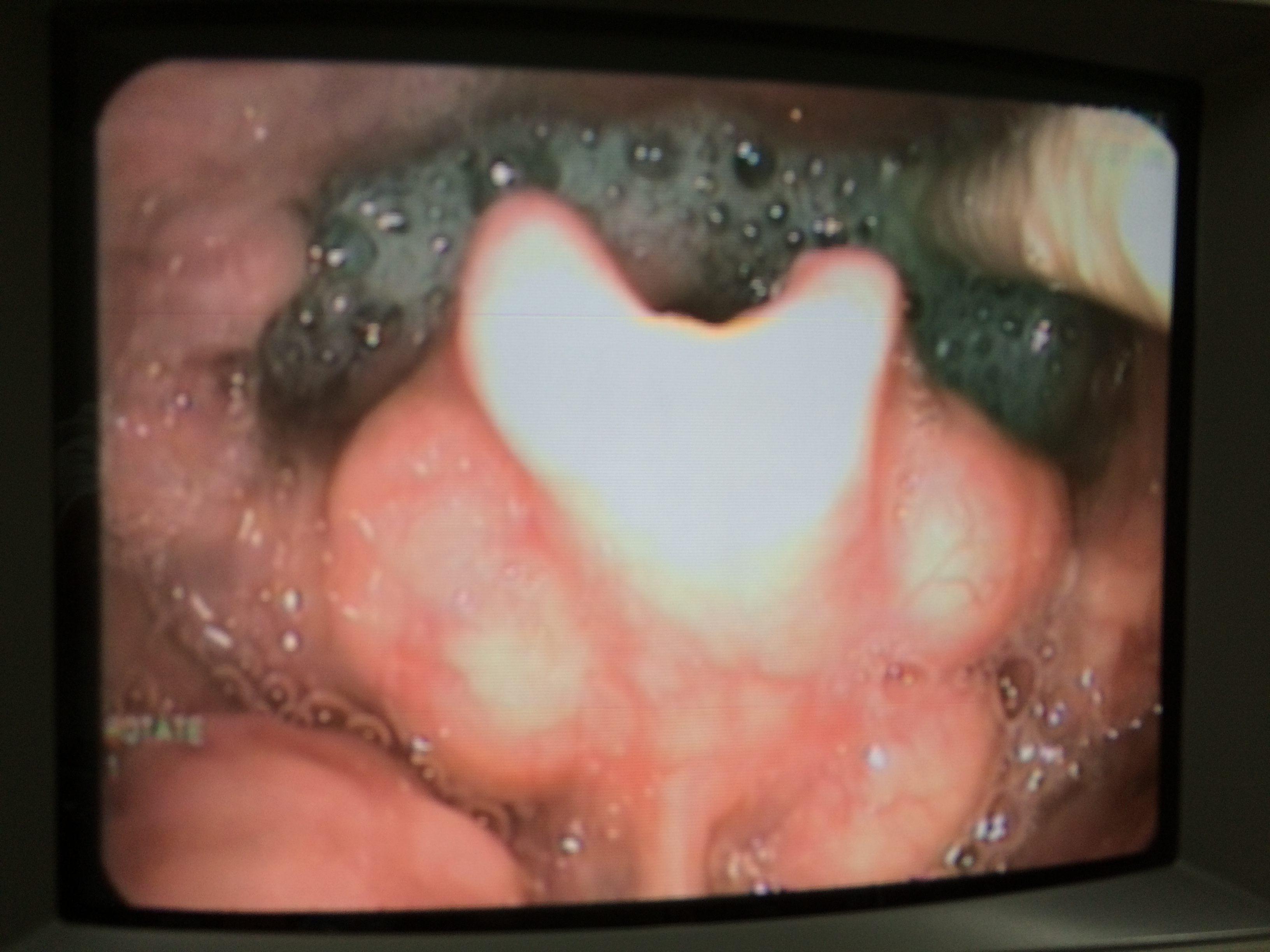
1) Most SLPs would want to refer the patient for an objective assessment [Videofluoroscopy (VFS) or Fiberoptic Endoscopic Examination for Swallowing (FEES)].
2) Some would want to downgrade the diet accordingly to patient’s presentation and observe as so far no other professionals have reported any significant changes.
3) Some would want to inform the team doctor regarding the worsening dysphagia, and to rule out the potential underlying medical complications.
I asked my SLP colleague the following questions:
Question 1: What are the possible causes of worsening dysphagia?
Answer: Maybe stroke, and maybe other new neurological deficits.
Question 2: Why do you think no one else notice any other changes in status except you?
Answer: Not sure. That’s why I am worried that I am wrong.
My answer: Pt is dense hemiplegia (power = 0), and globally aphasia. Unlikely for anyone else to have noticed any changes functionally as both limbs and language functions are 0.
Question 3: What would be your recommendation?
Answer: What if I am wrong? I don’t dare to ask for a CT scan or MRI as I could be wrong and patient may end up paying for unnecessary procedure and it is not cheap.
Question 4: What if you are right?
Answer: Then the medical team can treat the pt earlier.
Question 5: Now evaluate the pro and cons the decision “what if you are wrong?” vs “what if you are right?”.
Answer: Ok I think it would be better to discuss with team doctor and seek their opinion on this. Will suggest further assessment to rule out new events (such as stroke / neuro issues)
After discussion with the doctor, patient was sent to the acute hospital for urgent CT scan. The new CT scan showed hemorrhagic conversion on the left MCA infarct (worsening of the stroke).
In summary, when we encounter rapid progression of dysphagia, perhaps it would be better to speak to the team doctor to find out the cause(s). Objective swallowing assessment may want to be held off until patient’s medical status is stabilized.